|
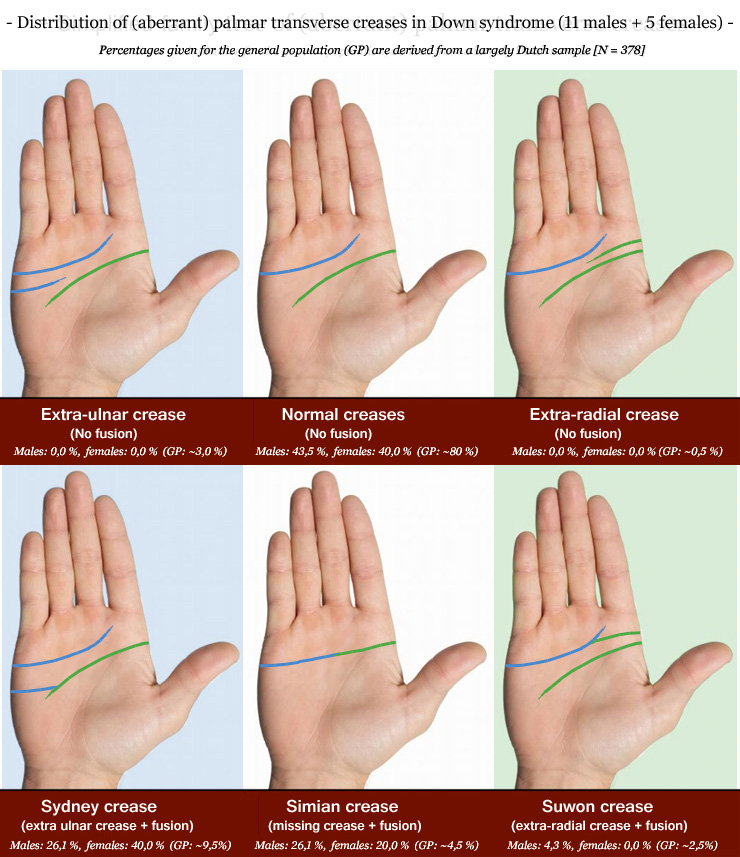
JULY 18, 2017 Distribution of palmar transverse creases in Down syndrome!The significance of the palmar transverse creases became initially well known due to the association of the simian crease with Down syndrome (trisomy 21). Later, a likewise relationship was described for the Sydney crease. However, both the simian line & Sydney line are also found with a much lower prevalence in the general population; this raises the question what exactly makes the palmar creases significant for Down syndrome. In this article the new family tree of aberrant palmar transverse creases (2017) is used to explore this from bottom to top with all attention initially focussed on just the interaction between distal transverse creases and the proximal transverse creases involving both hands together.The picture at the top of this articel presents the distribution of the 6 major categories in the simple version of the family tree for a Down syndrome sample involving 16 subjects; the picture displayed below presents the distribution of the 25 subvariants for the advanced version of the family tree. Both pictures present the numbers for in respective males and females separately, and both pictures also display between parentheses the estimated percentage for the general population. An analysis of the details is presented below involving 4 elements, which together lead to a complex constellation that is seen in almost half of the subjects in the Down syndrome sample. 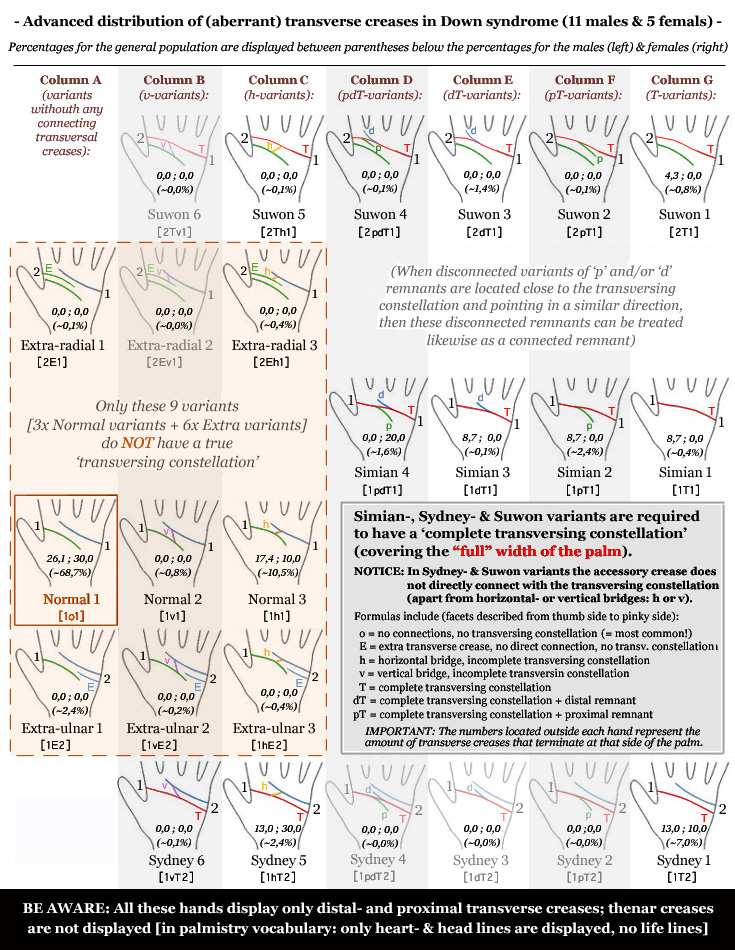
in both Down syndrome males & females The distribution of transversal creases in the simple version of the family tree (displayed at the top of this article) shows that in both Down syndrome males & females the significance of especially the simian crease (males & females: 24,24%) and also the Sydney crease (males & females: 30.3%) is confirmed (GP: simian crease 4,5% & Sydney crease 9,5%). And it is also not surprizing to notify as well that in both Down syndrome males & females the prevalence of normal variations is only about half of the prevalence in the general population (males: 43% & females: 40%, versus GP: 80%). The distributions displayed in the advanced family tree show that for only 3 individual sub-variants a very consistent & significant difference becomes manifest (against estimated values for the general population): DS-trend I - The largest effect becomes manifest in 'Sydney 5' variants, which involves a Sydney line featured with a horizontal bridge (h-variant) between the two creases; with an average percentage of 18,18% the prevalence of 'Sydney 5' variants is 7,5x higher compared the estimated prevalence for the general population (2,4%). Additionally, it is also interesting here to notify that the prevalence of h-variants is 2.4x higher in Down syndrome (33,3%) versus the normal population (13,8) - though this effect can largely be attributed to the Sydney 5 variant. DS-trend II - The prevalence of another Sydney crease variant - 'Sydney 1' - is also consistently higher in both Down syndrome males (13,0%) and Down syndrome females (10,0%); the average is here almost 75% higher than the estimated prevalence for the general population (7,0%). DS-trend III - Finally, the prevalence of 'Normal 1' variants is also consistently lower in both Down syndrome males (26,1%) and Down syndrome females (30,0%), versus a much higher estimated prevalence for the general population (68,7%). NOTICE: Special attention appears also appropriate for the prevalence of 'Simian 3' variants, spotted in 2 Down syndrome males (= 18,18% of the DS males, or 12,5% of the total DS population) versus a zero prevalence in the rest of the research population (= 0,0%); the prevalence of 'Simian 1' variants in the Down syndrome sample is also considerable - though only spotted in both hands of 1 male (= 6,25%), in the rest of the research population this simian line variant in both hands has been spotted only once in a male Bachelor student (= 0,28% of research population without DS). This suggests that not all 4 simian line variants have equal significance for Down syndrome. Also, be aware that 'Normal 3' is relatively common in the general population; after the 'Normal 1' variant it has in most populations the highest prevalence (near 10%, variations between 6% and 15% are also normal), in Down syndrome the prevalence is at the higher end just outside the normal range (15,2%). 
in both Down syndrome males & females Another effect, which has never been notified in the literature involving the palmar creases in Down syndrome, involves the lack of symmetry between both hands - especially involving the normally by far most common 'Normal 1' variant. The impact of this effect manifests via the following 3 Down syndrome trends: DS-trend IV - First of all, even though in the studied population none of the Down syndromes males nor females has a 'Normal 1' in both hands, 4 of the 16 Down syndrome subjects do have 'Normal 1' combined with 'Normal 3' (= 25,0%, versus 8.0% in the GP). The next paragraph will show that the significance of this combination especially becomes manifest when in both hands the proximal transverse crease (a.k.a. head line) is also connected with the thenar crease (a.k.a. life line), or at least in one of both hands the connection is very long and extended to (or beyond) the vertical plain of the interdigital zone between the index- and middle finger. DS-trend V - A 'Normal 1' constellation in both hands was not observed in the Down syndrome sample at all (= 0,0%); however, a considerable majority involving 201 out of 362 subjects in the research population except Down syndrome (= 55,5%) does have such a combination. Interestingly, among the samples included in the research population (21 sub-populations have been studied) there is actually just 1 other population where a likewise tendency has been noticed: among a sample of 11 subjects with heart conditions (none of them have Down syndrome) there is only 1 subject who has a 'Normal 1' constellation in both hands. This is particularily interesting in the perspective of the fact that statistics in general indicate that a small majority of people with Down syndrome is known to have a heart condition. DS-trend VI - In the studied Down syndrome sample right-left symmetry is only observed when both hands are featured with a similar simian crease variant, or a similar Sydney crease variant. Interestingly, in the heart conditions sample (N=11) there are only two subjects with right-left symmetry; one subject has 'Sydney 1' variants in both hands, the other subject has 'Normal 1' in both hands. proximal transverse crease & thenar crease!
DS-trend VIII - In total 12 of the 32 Down syndrome hands (37,5%) have a 'long closed' terminating proximal crease, but only 2 hands (6,25%) are also featured with 'Normal 1' (both have it in the right hand; one of both subjects has a 'Simian 1' in the left hand and the other has a 'Normal 3' in the left hand). In the remaining subjects of the research population 86 out of 362 (23,8%) have a 'long closed' terminating proximal crease, and 112 subjects (15,5%) have it combined with 'Normal 1'. DS-trend IX - Right-left asymmetry is spotted for the radial termination of the proximal creases in 4 of the 16 studied Down syndrome subjects (25,0%); in all 4 subjects (25%) one of both hands has a 'long closed' termination point. In the remaining subjects of the research population 140 out of 362 (38,7%) have right-left asymmetry, and 74 subjects (20,4%) have it combined with 'Normal 1'. Almost half of the Down syndrome sample is featured in at least 1 hand with a strong extra hypothenar crease (featured with a structure similar to the major creases) located halfway the hypothenar zone at the ulnar side; in two subjects it is present in both hands. combined with a Sydney- or simian crease in the same hand is very signficant for Down syndrome! 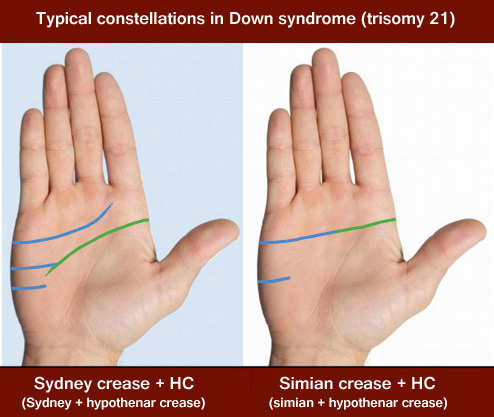
Via the 4 elements discussed above a highly signficant constellation has been identified involving a strong extra crease (featured with a structure similar to the major creases) located halfway at the ulnar side of the hypothenar zone and terminating at the side of the palm (HC = hypothenar crease), combined with a 'closed' simian- or Sydney crease - see picture above where both constellations have been labeled as 'Sydney crease + UC' & 'simian crease + UC', for each variant is also a Down syndrome example displayed below. A fundamental difference between this hypothenar crease and an 'extra-ulnar crease' is that the latter is typically found in the upper quarter of the hypothenar zone (usually above the termination point of the proximal transverse crease). This constellation has been observed in 7 out of 16 Down syndrome people (43,7%), in all cases present in just one of both hands but the other hand also has a 'closed' proximal crease termination, connecting with the thenar crease. The prevalence of this complex constellation is much lower in the other sub-groups in the rest of the research population, it is found in only 2,8% (10 out of 362 subjects). 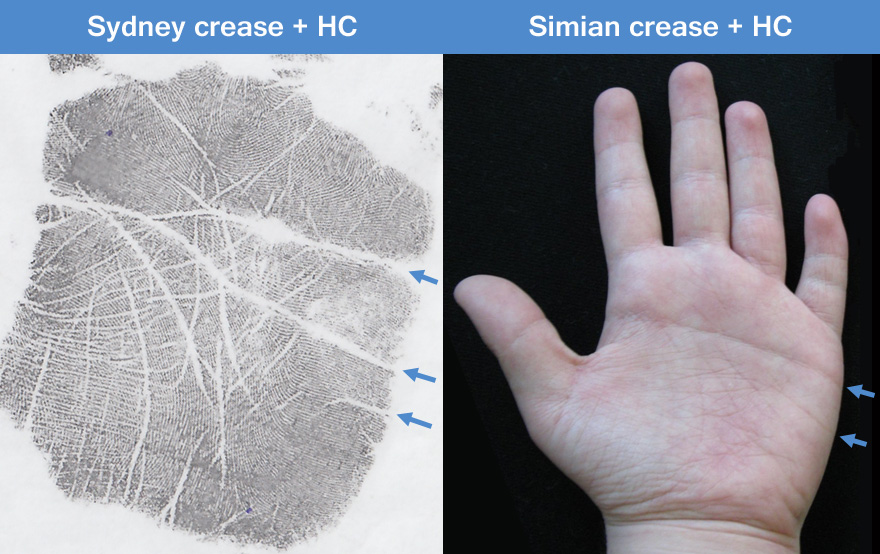
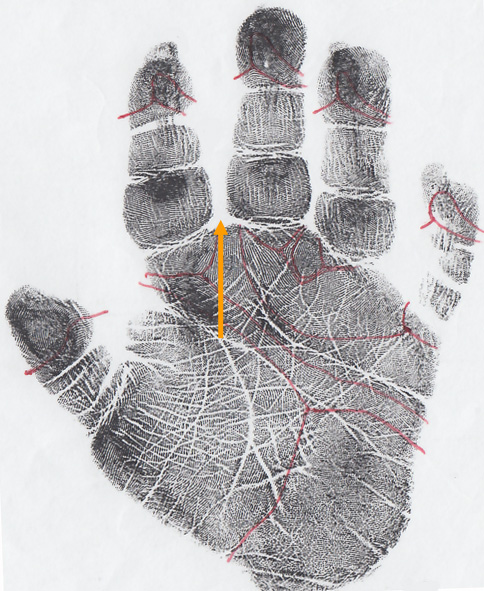
Interestingly, the significance of this complex constellation for Down syndrome becomes even more appartent when the combination of both hands is taken in consideration. In 5 of the 16 Down syndrome subjects (31,2%) the constellation typically has a characteristic seen in one of the columns E, F or G in the advanced family tree; the other hand is also typically featured with a constellation that is asymmetric for multiple aspects without the involvement of a Suwon crease, Extra-ulnar crease nor Extra-radial crease; and both hands typically have a normal 'closed' proximal crease termination. In all 5 of the Down syndrome cases at least 2 out of 3 additional requirements are present. In the rest of the research population (N=362) these criteria are only met in a single person who has autistic spectrum disorder, resulting in a prevalence for the rest of the research population of just 0,3% versus a prevalence of 31.2% in Down syndrome! NOTICE: Finally, it is also of fundamental importance that the (extra) hypothenar crease may be understood to represent a 'shift' that sort of compensates for another typical phenomenon that is often present on the ulnar side of the hand in Down syndrome: a single 5th digit crease (see picture below); the compensation can be described here to represent a crease-related-shift from the pinky finger to the hypothenar zone. 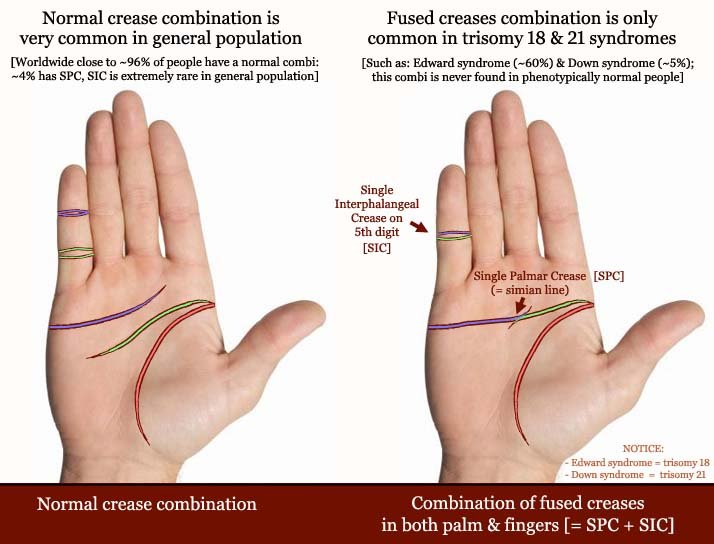
The simian line (or Sydney line) in Down syndrome is also often featured with a single 5th digit crease. |
|
|
© COPYRIGHT 2002-2017: |